
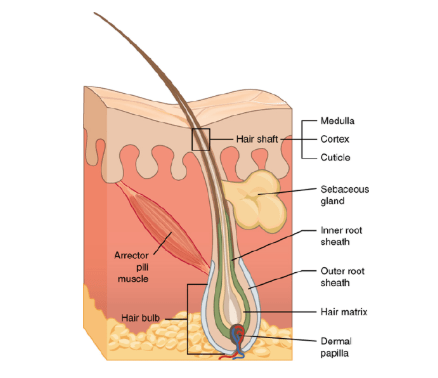
The pilosebaceous unit (PSU), consisting of a hair follicle, sebaceous gland, and arrector pili muscle, is essential for skin protection, lubrication, and sensory functions. It acts as a dynamic mini-organ within the skin, responding to hormones and microbes while maintaining barrier integrity. Variations in PSU size and activity influence conditions like acne, affecting up to 95% of adolescents globally.
Detailed Anatomy
The hair follicle divides into regions: infundibulum (surface opening), isthmus (mid-portion), and inferior segment (bulb with matrix cells for hair growth). Terminal follicles extend into the subcutis for thick hairs, while vellus ones remain superficial. The arrector pili muscle attaches obliquely, enabling “goosebumps” for thermoregulation and sebum dispersion.
Embryonic Development
PSU formation starts at 8-12 weeks gestation with epidermal placodes interacting with dermal papillae, guided by HOX genes and signaling pathways. Sebaceous glands mature by 13-15 weeks under maternal androgens, producing sebum as the fetus’s first glandular output by week 17. This intrinsic patterning determines lifelong androgen sensitivity.
Sebum Production and Composition
Sebaceous glands generate sebum—90% of skin lipids—including triglycerides (60%), wax esters, squalene (unique for antioxidants), and free fatty acids like oleic and palmitoleic. These lipids waterproof the skin, deliver antimicrobials (e.g., cathelicidin, hBD-2), and maintain acidic pH against pathogens. Postnatal sebum peaks early, quiets until puberty, then surges with adrenarche.
Hormonal Regulation
Sebocytes express androgen receptors and enzymes like 5α-reductase type 1, converting cholesterol or progesterone directly to potent DHT. Androgens drive hyperplasia and lipogenesis; local overproduction or hypersensitivity fuels acne without systemic hyperandrogenemia. Neuropeptides (e.g., substance P) further modulate cytokines and differentiation.
Microbiome and Immunity
Cutibacterium acnes (formerly P. acnes) dominates the lipid-rich PSU niche, producing short-chain fatty acids that inhibit biofilms and rivals like S. epidermidis. Dysbiosis favors inflammatory IA1 phylotypes in acne lesions, activating TLR2/CD14 on sebocytes. Sebum fatty acids enhance phagocytosis and hBD-2 against C. acnes, integrating innate defense.
Key Disorders of the PSU
Acne vulgaris is the most common PSU disorder, driven by hyperseborrhea, follicular hyperkeratinization, C. acnes dysbiosis, and inflammation. Rosacea involves pilosebaceous inflammation, often with higher Demodex folliculorum density triggering TLR2 responses and protease release. Folliculitis arises from bacterial (e.g., S. aureus), fungal (Malassezia), or parasitic (Demodex) invasion of follicles.
Acne Treatments
Guidelines recommend multimodal topical therapies first: retinoids (normalize keratinization), benzoyl peroxide (antibacterial), and topical antibiotics or azelaic acid for mild acne. Moderate cases add oral antibiotics (e.g., doxycycline); severe nodulocystic acne uses isotretinoin, which shrinks sebaceous glands. Hormonal agents like spironolactone or contraceptives target androgen effects in women.
Other PSU Disorder Management
For rosacea, topical ivermectin or metronidazole reduces Demodex and inflammation; oral tetracyclines help papulopustular types. Folliculitis treatment varies: antibacterials for staphylococcal, oral antifungals (itraconazole/fluconazole) for Malassezia, and ivermectin/permethrin for Demodex. Early intervention prevents scarring across these conditions.
Clinical Relevance
Grasping PSU disorders enables precise grading, tailored therapies, and patient education. Factors like genetics and diet modulate risks, emphasizing holistic care.
Conclusion
Acne ranks among the most common skin conditions from adolescence into adulthood, with the pilosebaceous unit driving its pathogenesis. A solid grasp of its anatomy and physiology proves essential for identifying acne types, assessing severity, and customizing treatments to match each patient’s needs and physiological state. These insights form the cornerstone of effective dermatological consultations.
References
- Kurokawa I, Danby FW, Ju Q, et al. New developments in our understanding of acne pathogenesis and treatment. Exp Dermatol. 2009;18(10):821-32.
- Zouboulis CC. The sebaceous gland. Hautarzt. 2010;61(6):467-8,470-4,476-7.
- Bhate K, Williams HC. Epidemiology of acne vulgaris. Br J Dermatol. 2013;168(3):474-85.
- Tan JK, Bhate K. A global perspective on epidemiology of acne. Br J Dermatol. 2015;172(suppl 1):3-12.
- “2020.3.2.pilosebaceous.” Our Dermatology Online. 2020. Available at: odermatol.com. [Pilosebaceous unit anatomy review]odermatol
- “Sex hormones and acne.” Clinics in Dermatology. 2017. Available at: sciencedirect.com. [Hormonal regulation]sciencedirect
- “Sebaceous-immunobiology is orchestrated by sebum lipids.” PMC. 2017. Available at: pmc.ncbi.nlm.nih.gov/articles/PMC5821166/. [Sebum lipids/immunity]pmc.ncbi.nlm.nih
- “Skin dysbiosis and Cutibacterium acnes biofilm.” Scientific Reports (Nature). 2022. Available at: nature.com/articles/s41598-022-25436-3. [Microbiome in acne]nature
- “Pilosebaceous Unit – an overview.” ScienceDirect Topics. Available at: sciencedirect.com/topics/veterinary-science-and-veterinary-medicine/pilosebaceous-unit. [Core PSU structure]sciencedirect
- “Acne Vulgaris – StatPearls.” NCBI Bookshelf. 2023. Available at: ncbi.nlm.nih.gov/books/NBK459173/. [Pathogenesis and treatments]

Leave a comment