
Acne is one of the most prevalent skin conditions in adolescent to adult age groups. If you are seeking the best acne treatment Mumbai has to offer, the experts at Glory Aesthetics are here to help you understand this condition and guide you toward clearer skin.
What is Acne?
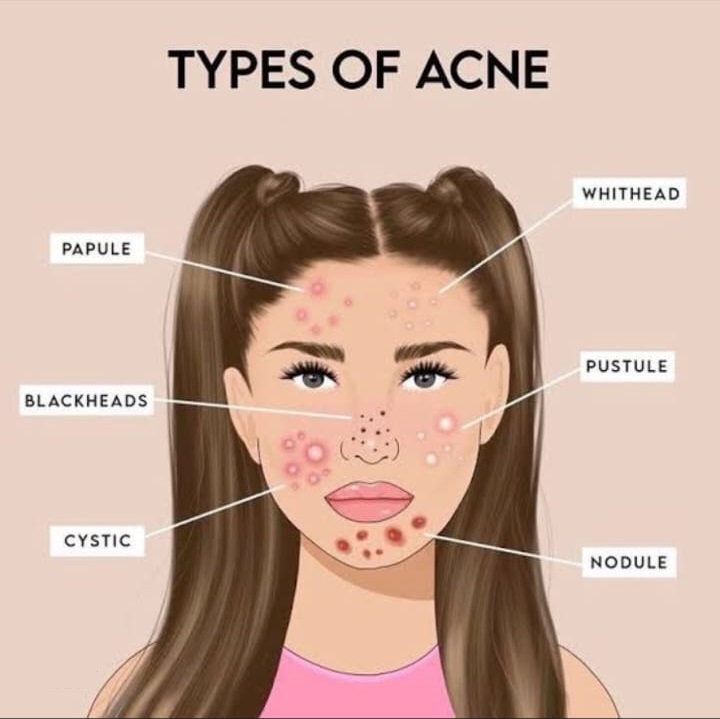
Acne is a disorder of the pilosebaceous unit, and it has a chronic but self-limiting course. Acne vulgaris is the commonest variant of acne and presents as pleomorphic lesions such as comedones, papules, pustules, nodules, cysts, and abscesses. The general population often terms acne vulgaris as pimples, blackheads, and whiteheads. These lesions predominantly occur in the seborrheic areas of the body including the face, neck, chest, and upper back.
Other clinical subtypes of acne include adult-onset acne, occupational acne, acne conglobate, and acne fulminans. Additionally, acne may develop in neonates due to maternal hormones; however, these lesions resolve spontaneously within six weeks.
[Visual Suggestion: Insert an infographic illustrating the different types of acne lesions like comedones, papules, and pustules.]
History
In the Ebers Papyrus dating 3400 BC, ancient Egyptians mentioned the term AKU-t to define an inflamed swelling or boil. Considering its phonetic resemblance to the currently used term acne vulgaris, it is likely to be the origin of the word acne. The term acne vulgaris was first introduced by Fuchs in 1840, where “vulgaris” means common.
Pathophysiology
To understand your specific acne causes, we must look at the pilosebaceous unit, which is the center of the pathomechanism of acne. Different inflammatory mechanisms cause the blockage of the sebaceous unit. There are four main pathogenic processes that drive the condition:
- Alteration of follicular keratinization.
- Increased and changed sebum.
- Production of normal levels of androgens – dehydroepiandrosterone.
- Follicular colonization with Propionibacterium acnes.
A high sebum concentration favors the growth of Propionibacterium acnes. This bacterial growth triggers the inflammatory process in acne leading to more severe acne.
Epidemiology
Acne is a very common condition with a lifetime prevalence of nearly 85% on a global scale. Acne predominantly occurs during adolescence, with most studies reporting a higher prevalence in females than males. The more common age is between 14 to 17 years old among girls , and 16 to 19 years old among boys. While acne may be self-limiting in the majority and resolve in their early and late twenties, it may persist into adult life. Acne persists into the 20s for 64% of individuals , into the 30s for 43% of individuals , and late adult-onset acne over 25 years of age affects 8.4%.
[Visual Suggestion: A gentle, lifestyle photo of a young adult looking confidently into the mirror, or a chart showing the age-based prevalence of acne.]
Risk Factors
Individuals of Asian and African ethnicities tend to develop higher grades of acne compared to the white population where mild acne is more common. Adult-onset acne is characterized by lesions predominantly affecting the lower third of the face including the jawline. A variety of epidemiological factors are associated with increased sebum secretion and breakouts:
- Hormones, Age, and Gender: Female gender and the adolescent/late teens/young adult age are key epidemiological factors. As sebum production increases with puberty, older teenagers produce higher sebum compared to younger teenagers. During the premenstrual phase of the menstrual cycle, around 70% of affected females report a premenstrual flare of acne due to edema of pilosebaceous ducts.
- Genetics and Ethnicity: A family history of acne in first-degree relatives is mostly present in 80% of cases. Asian and African ethnicities are also significant factors.
- Weight and Diet: Obese or overweight individuals with higher glycemic loads and higher androgen levels have increased sebum secretion. Thus, a higher body mass index promotes the formation of more acne lesions. A high glycemic index and high glycemic load of food influence breakouts. Consuming food, dairy products, junk food, and milk increases tissue levels of 5 alpha dihydrotestosterone.
- Skin and Cosmetics: Oily skin and occlusive cosmetic usage are recognized contributors.
- Psychological Factors: Anxiety, stress, and anger are notable factors. Anxiety, stress, and anger may aggravate acne lesions stimulating cortisol hormones. In cases of mental stress, the production of neurotransmitters like P is higher which stimulates sebum production.
- Medical Conditions and Interventions: Polycystic ovarian syndrome or disease triggers acne. Medical products like oral contraceptive pills , oral topical corticosteroids , and compounds like bromides, iodides, lithium, or dioxide are epidemiological factors.
Quality of Life Impact
Acne and its sequelae adversely affect the quality of life of an individual. The lesions may heal with post inflammatory hyperpigmentation (PIH) and scars. In general, the darker skin population often develops PIH , and nearly 20% of affected patients develop severe acne which leads to scarring. While assessing a patient with acne, it is very important to identify the type of acne, grade its severity, and also assess the psychological impact it has on the patient.
Ready to start your journey toward clear, healthy skin? Book a consultation at Glory Aesthetics today.
References
- Grant RN. History of acne Proc R Soc Med. 1951:44:647-52.
- Kurokawa I, Danby FW, Ju Q, et al. New developments in our understanding of acne pathogenesis and treatment. Exp Dermatol 2009:18(10):821-32.
- Zouboulis CC, The sebaceous gland. Hautarzt. 2010;61(6):467-8,4704,476-7.
- Bhate K, Wiliams HC. Epidemiology of acne vulgaris Br J Dermatol. 2013:168 (3) : 474 -85.
- Burton JL, Cunliffe WJ, Stafford L. The Prevalence of acne vulgaris in adolescence Br J Dermatol 1971:85 (2) 119 -26.
- Tan JK, Bhate K.A global perspective on epidemiology of acne. Br J Dermatol. 2015:172(suppl 1):3-12.
- Goulden V , Clark SM, Cunliffe W J post adolescent acne a review of clinical features Br Dermatol. 1997 : 136 (1) : 66 -70.
- Poli F , Dreno B, Verschoore M. An epidemiological study of acne in female adults: Results of survey conducted in France J Eur Aced Dermatol Venereol. 2001:15 (6):541-5.
- Ghodsi SZ, Orawa H , Zovboulis CC . Prevalence severity and severity risk factors of acne in high school pupils. Community based study. J invest Dermatol. 2009:129 (9) : 2136-41.
- Karciauskiene J, Valiukeviciene S, Gollnick H , et al. Prevalence and risk factors of adolescent acne among school children in Lithuania: cross sectional study J Eur Aced Dermatol Venereol. 2014:28(6):733-40.
- Ayer J Burrrows N Acne More than skin deep. Postguard Med J. 2006:82 (970): 500-6.

Leave a comment